
The Aged Care Act 2024 has fundamentally shifted what it means to lead an aged care organisation. Aged care governance obligations for executives are no longer a background administrative function. They are statutory duties with real consequences, and the sector is still catching up. If you are an executive or board member trying to balance mounting compliance demands with the day-to-day pressure of running quality services, this guide is written for you. We will cover what the law actually requires, how to build systems that work, and where most organisations quietly go wrong.
Table of Contents
- Key takeaways
- Aged care governance obligations executives must understand first
- Executing governance obligations step by step
- Common pitfalls in governance compliance
- Verifying and sustaining governance over time
- My perspective: governance as leadership, not paperwork
- How Theplanningandpracticehub can support your governance
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Statutory duties are non-delegable | Executives hold personal legal responsibility under the Aged Care Act 2024 that cannot be passed down the chain. |
| Board skills must match governance demands | Clinical, financial, risk, and consumer expertise are all required on a well-functioning aged care board. |
| Clinical governance belongs at board level | Monthly reporting on incidents, care minutes, and quality metrics is a board-level obligation, not just a management task. |
| Reactive compliance costs more than prevention | Organisations trapped in compliance cycles lose capacity for strategic planning and quality improvement. |
| Verification requires independent scrutiny | Internal audits and peer reviews are necessary to validate governance beyond self-assessment. |
Aged care governance obligations executives must understand first
The term "governance obligations" covers a lot of ground. In the aged care context, the recognised industry framework is statutory governance duty, and it sits at the intersection of legal accountability, clinical oversight, and organisational leadership. Under the Aged Care Act 2024, responsible persons hold non-delegable duties of due diligence. That means you, as an executive, are personally accountable for ensuring your organisation meets its obligations around care recipient safety, workforce standards, and regulatory compliance.
These are not obligations you can hand to a compliance officer and consider resolved. The Act specifically requires that responsible persons take active steps to understand risks, monitor performance, and intervene when things go wrong.
Building the right board for the job
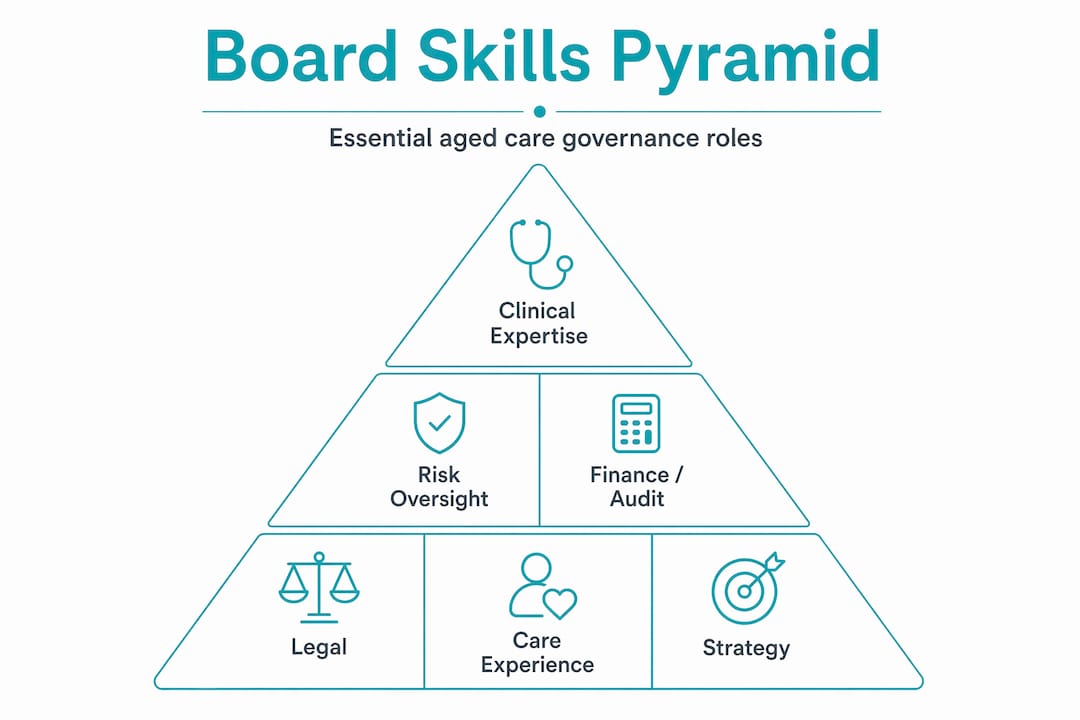
Governance starts with who is in the room. A board that lacks clinical expertise cannot meaningfully interrogate care quality data. A board without financial acumen cannot assess whether resource allocation decisions are sustainable. Board skills matrices that map competencies against governance needs are now considered standard practice, with essential areas including aged care operations, clinical governance, financial management, risk, human resources, and consumer engagement.
Getting this right is not a one-time exercise. Skills gaps change as the regulatory environment changes. Review your board composition at least annually against what the organisation actually needs.
Governance infrastructure that holds up under scrutiny
Beyond people, you need systems. Effective governance infrastructure includes:
- A board charter that clearly defines roles, responsibilities, and decision-making authority
- A conflicts of interest register that is actively maintained and reviewed, not filed and forgotten
- A delegation schedule that specifies what decisions sit at board level versus management level
- A succession plan for both board and executive leadership
- A compliance monitoring system that tracks obligations in real time
Integrated dashboards that bring together risk, clinical, and compliance data in one place are increasingly recommended to prevent fragmented reporting and executive overload.
Pro Tip: Do not build your governance framework around what the regulator asks to see. Build it around what you need to actually run the organisation well. Compliance visibility will follow.

Executing governance obligations step by step
Knowing what is required is one thing. Putting it into practice consistently is where most organisations struggle. Here is a structured approach to executing your governance duties.
-
Establish a responsible persons register. Document every person who holds a responsible person role, including their suitability assessment status. This register must be current and accessible for regulatory review at any time.
-
Monitor workforce compliance actively. The 215 care minutes target and 24/7 registered nurse coverage requirements are board-level concerns, not just operational ones. Your reporting systems must surface compliance or non-compliance clearly and promptly.
-
Embed clinical governance into board reporting. Monthly clinical governance reports should cover Serious Incident Response Scheme notifications, complaints received and resolved, medication errors, falls data, and care quality metrics. Boards that receive this information regularly are far better positioned to fulfil their due diligence duties.
-
Develop a reporting cadence that covers all domains. Monthly dashboards should address clinical performance, operational metrics, financial position, and compliance status. This is not about creating paperwork. It is about giving the board the information it needs to govern.
-
Treat consumer rights as a governance matter. Complaints management is not just a service quality issue. It is a governance obligation. Your board should receive regular reports on complaint volumes, themes, and resolution outcomes.
-
Use escalation protocols deliberately. When risks are identified, your governance framework must specify who is notified, in what timeframe, and what remediation looks like. Board minutes should show active risk identification and remediation decisions, not passive awareness.
-
Build a culture of active oversight. Governance treated as a formality is governance that fails when it matters most. The board's role is to ask hard questions, not to ratify management decisions.
Pro Tip: Schedule a standing agenda item at every board meeting for clinical governance reporting. If it is not on the agenda, it will not get the attention it deserves.
What good reporting actually looks like
| Reporting domain | Frequency | Key metrics |
|---|---|---|
| Clinical governance | Monthly | SIRS incidents, falls, medication errors, care minutes |
| Workforce compliance | Monthly | Registered nurse hours, care minute targets, vacancies |
| Financial performance | Monthly | Budget variance, liquidity, capital expenditure |
| Complaints and consumer rights | Monthly | Volume, themes, resolution timeframes |
| Risk register | Quarterly | Open risks, ratings, remediation status |
Common pitfalls in governance compliance
Understanding what can go wrong is as useful as knowing what to do right. These are the patterns we see most often in aged care organisations struggling with governance.
-
Reactive compliance culture. When governance activity is driven entirely by regulator requests or incidents, the organisation is always behind. Leaders trapped in reactive cycles lose capacity for long-term planning, and the workforce follows suit. The result is an organisation that manages crises rather than prevents them.
-
Fragmented reporting systems. When clinical data lives in one system, financial data in another, and compliance records in a spreadsheet, no one has a complete picture. This is how risk blind spots form.
-
Delegating clinical governance without board engagement. Clinical governance cannot be fully delegated to management. Boards that remain distant from clinical quality have historically been associated with provider failures. The board must receive, interrogate, and act on clinical data.
-
Poor documentation and missing audit trails. When the regulator comes calling, what matters is what you can demonstrate. Verbal decisions, undocumented risk discussions, and incomplete board minutes are liabilities.
-
Insufficient board diversity. A board that is homogenous in background and expertise will have blind spots. This is not just a governance risk. It is a strategic one.
"Governance challenges are amplified for smaller providers who often lack dedicated governance staff, necessitating clear guidance and support." — Australian Ageing Agenda
Smaller organisations face a particular challenge here. The governance burden is the same regardless of size, but the internal resources to manage it are not. This is where external support and clearly structured frameworks become genuinely useful rather than optional.
Verifying and sustaining governance over time
Getting governance right once is not the goal. Sustaining it is. These practices help organisations move from initial compliance to continuous improvement.
-
Annual board self-assessments. Every board should formally assess its own performance against its charter and governance obligations. This is not a rubber stamp exercise. It should surface genuine gaps and lead to concrete development actions.
-
Skills matrix reviews. Essential competencies for aged care boards include clinical governance, financial management, risk, and consumer engagement. Review your matrix annually and recruit or develop accordingly.
-
Independent audits and peer reviews. Internal self-assessment has limits. External peer reviews and independent audits validate whether your governance is actually working, not just whether it looks like it is on paper.
-
Embedding governance into workforce systems. Governance culture does not live only at board level. It needs to be reflected in how managers are assessed, how staff are inducted, and how quality improvement is structured across the organisation.
-
Succession planning for leadership continuity. Leadership in aged care now requires active succession planning, particularly given workforce shortages. A governance framework that depends on specific individuals is fragile.
Pro Tip: Treat the Aged Care Quality Standards as a living operational framework rather than a static checklist. Organisations that do this consistently report better readiness for regulatory review and fewer reactive scrambles.
| Verification activity | Recommended frequency | Responsible party |
|---|---|---|
| Board self-assessment | Annual | Board chair |
| Skills matrix review | Annual | Governance committee |
| Internal compliance audit | Bi-annual | Management with board oversight |
| Independent governance review | Every two years | External reviewer |
| Regulator readiness check | Ongoing | Executive team |
My perspective: governance as leadership, not paperwork
I have worked alongside aged care boards and executives for nearly three decades, and I want to say something that does not get said enough. The governance reforms are not the problem. The problem is how we have been conditioned to respond to them.
I have seen organisations spend enormous energy producing governance documentation that no one reads and reporting that no one acts on. The compliance fatigue is real. 55% of providers report reluctance to continue service delivery because of governance and compliance complexity. That statistic should concern all of us, but the answer is not less governance. It is better governance.
What I have learned is that the organisations doing this well are not the ones with the most sophisticated systems. They are the ones where the board genuinely understands its role and takes it seriously. Where the CEO and board chair have a trusting, honest relationship. Where clinical governance is not a quarterly agenda item but a thread running through every board conversation.
The shift from passive compliance to active stewardship is not a structural change. It is a cultural one. And culture starts with leadership visibility. When executives treat governance as a genuine expression of organisational values rather than a regulatory imposition, the workforce notices. Quality follows.
My practical advice: stop asking "what does the regulator want to see?" and start asking "what do we need to know to lead this organisation well?" The answers are usually the same. But the second question produces governance that actually works.
— Rachel
How Theplanningandpracticehub can support your governance
Translating governance obligations into day-to-day practice is where many aged care organisations get stuck. Knowing the requirements is one thing. Building the systems, culture, and documentation to meet them consistently is another challenge entirely.
At Theplanningandpracticehub, we work directly with aged care executives and boards to develop governance frameworks that are practical, not theoretical. Founded by Rachel Willis, with nearly three decades of experience across human services and regulatory compliance, the Hub offers tailored NFP governance consulting that reflects the real pressures organisations face under the Aged Care Act 2024. Whether you need help building your board charter, establishing clinical governance reporting, or preparing for a regulatory review, our consulting services are designed to meet you where you are and move you forward.
FAQ
What are the non-delegable duties under the Aged Care Act 2024?
Responsible persons hold personal statutory duties of due diligence that cannot be assigned to others. These include ensuring care recipient safety, meeting workforce obligations such as the 215 care minutes target, and maintaining active oversight of compliance across all domains.
How often should boards receive clinical governance reports?
Monthly reporting is the recommended standard, covering Serious Incident Response Scheme notifications, complaints, medication errors, falls data, and care minutes compliance. Boards that receive this information regularly are better positioned to fulfil their due diligence duties.
What is a responsible persons register?
A responsible persons register documents every individual holding a responsible person role within an aged care organisation, along with their suitability assessment status. It must be kept current and available for regulatory review at any time.
How can smaller providers manage governance obligations without dedicated staff?
Smaller providers can prioritise a clear governance framework with structured templates, external consulting support, and integrated reporting tools that reduce administrative burden. External peer reviews and governance partnerships offer a practical way to access expertise without building a large internal team.
What is the difference between clinical governance and general governance?
General governance covers the full scope of board oversight including financial, legal, risk, and operational accountability. Clinical governance is a specific subset focused on the quality and safety of care delivery, including incident management, care standards, and workforce clinical performance. Both are statutory obligations for aged care boards.